
1. Introduction
- The femur is the longest and strongest bone in the human body.
- It is located in the thigh, connecting the hip (proximal) to the knee (distal).
- Classified as a long bone (diaphysis + two epiphyses).
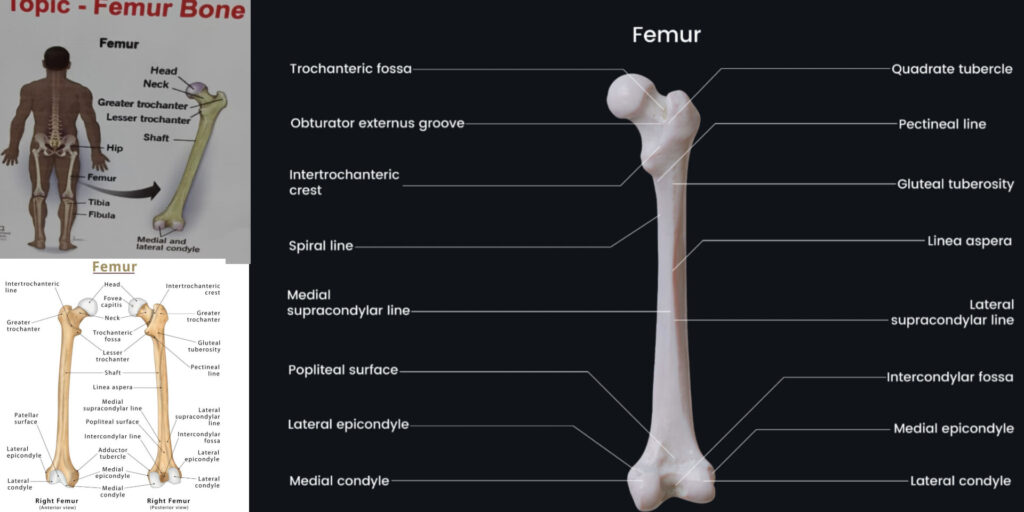
2. Anatomical Features of Femur
A. Proximal End
- Head
- Spherical and covered with hyaline cartilage.
- Articulates with the acetabulum of the hip bone (forming the hip joint).
- Contains the fovea capitis (a small pit for the ligamentum teres).
- Neck
- Connects the head to the shaft.
- Angle of inclination: ~125° (less in females).
- Common fracture site (especially in osteoporosis – femoral neck fracture).
- Greater Trochanter
- Large, lateral projection.
- Attachments:
- Gluteus medius & minimus (lateral surface).
- Piriformis (upper border).
- Lesser Trochanter
- Smaller, medial & posterior projection.
- Attachments:
- Iliopsoas tendon (major flexor of the hip).
- Intertrochanteric Line (Anterior) & Crest (Posterior)
- Line (anterior): Attachment for the iliofemoral ligament.
- Crest (posterior): Attachment for the quadratus femoris.
B. Shaft (Body)
- Triangular in cross-section (with Linea aspera – a rough ridge posteriorly).
- Attachments:
- Vastus lateralis & medialis (along margins).
- Adductor muscles (insert into linea aspera).
- Pectineus (spiral line).
C. Distal End
- Medial & Lateral Condyles
- Articulate with the tibia (forming the knee joint).
- Intercondylar fossa separates them posteriorly.
- Epicondyles
- Medial epicondyle: Adductor magnus attachment.
- Lateral epicondyle: Fibular collateral ligament attachment.
- Patellar Surface
- Smooth anterior surface for articulation with the patella.
3. Blood Supply of Femur
- Major sources:
- Medial & lateral circumflex femoral arteries (from profunda femoris).
- Nutrient artery (enters at linea aspera).
- Femoral head blood supply:
- Retinacular arteries (from circumflex femorals) – most important.
- Artery of ligamentum teres (minor role).
Clinical Note:
- Femoral neck fractures can disrupt blood supply → avascular necrosis (AVN) of the femoral head.
4. Ossification of Femur
- Primary ossification center: Shaft (8th week of fetal life).
- Secondary centers:
- Head (~1 year).
- Greater trochanter (~4 years).
- Lesser trochanter (~12 years).
- Fusion: ~18 years (all centers fuse).
5. Clinical Correlations
A. Femoral Fractures
- Neck of Femur Fracture
- Common in elderly (osteoporosis).
- Garden’s classification used.
- Risk of AVN due to disrupted blood supply.
- Intertrochanteric Fracture
- More stable (better blood supply).
- Treated with dynamic hip screw (DHS).
- Shaft Fracture
- Due to high-energy trauma.
- Deformity: Shortening, external rotation (due to muscle pull).
B. Hip Dislocation
- Posterior dislocation (common in car accidents).
- Signs:
- Limb shortened, adducted, internally rotated.
- Sciatic nerve injury possible.
C. Trendelenburg Gait
- Due to weak gluteus medius (attaches to greater trochanter).
- Pelvis drops on the opposite side during walking.
6. Mnemonics
- “Piriformis sits on Greater Trochanter” → Piriformis inserts on the upper border of GT.
- “Linea aspera = Adductor highway” → Adductor muscles attach here.
- “Femoral head blood supply: Retinacular is critical!”
7. Summary Table
| Part | Key Features | Clinical Importance |
|---|---|---|
| Head | Articulates with acetabulum | AVN in neck fractures |
| Neck | Connects head to shaft | Common fracture site (elderly) |
| Greater Trochanter | Gluteus medius/minimus attachment | Trendelenburg gait if weak |
| Lesser Trochanter | Iliopsoas insertion | Hip flexor strength |
| Linea aspera | Adductor muscle attachments | Shaft fractures → deformity |
Final Notes for Exams
- Longest bone in the body.
- Common fracture sites: Neck, intertrochanteric, shaft.
- Blood supply critical for femoral head survival.
- Hip vs. Knee joints: Proximal & distal articulations.